

Where are the best — and worst — states for women?
As a woman, do you ever consider which states you’d have a better chance of living in an emergency? The usual suspects rank in the bottom; some seem to intentionally plan to stay there.

One of the problems of being in health care is that you know too much. So, yes, when I consider vacations, I also have a list in the back of my mind of states where I’d have a significantly better chance of living than dying in an emergency. Women in the US face a growing number of threats to our health and well-being—and some states are more interested in raising the bar than others. I favor those.
The best and worst states for women and our health
WalletHub recently rated the best states for women, looking at the median earnings for female workers, share of women per state living in poverty, the unemployment rate among women, quality of women's hospitals, reproductive policies and access, uninsured rate among women, and female homicide and rape rates. Massachusetts came out on top, followed by Minnesota, Vermont, Maine, Maryland, NY, Hawaii and NJ.
The Commonwealth Fund, a foundation focused on health issues, focused more deeply on health care, scoring 32 measures of care access, quality, and health outcomes for women in their 2024 State Scorecard on Women’s Health and Reproductive Care. Massachusetts, which routinely scores high in healthy states for both men and women, came out on top again in this one, followed by New Jersey, Connecticut, Vermont, Hawaii, and New York.
In both the WalletHub and The Commonwealth Fund studies, the worst states for women include Oklahoma, Mississippi, Arkansas, Oklahoma, Alabama, and Louisiana. As a women’s health care consultant, I’ve done business in all of them and 42 other states; the ratings are right.
In the past, low-ranking states have often defended their position by claiming that better outcome states have more homogenous populations. Vermont is homogenous, but California, Hawaii, NJ and NY are some of the least homogenous states in the country. And on issues like our internationally-embarrassing, 80% preventable maternal death rate, California—the safest state for moms to have babies in the nation—has repeatedly shown that if a state commits to improving women’s health, it can and will, quite quickly.
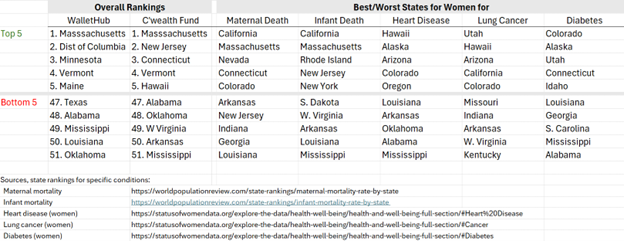
Deaths from all causes among women of reproductive age — 15 to 44 — are highest in southeastern states—our ‘neonatal death belt.’ The lowest performers are Mississippi, Texas, Nevada, and Oklahoma. Tennessee, Mississippi, and Louisiana have our worst maternal death rates despite the presence of some great health systems…at least for some of the population.
Infant deaths go hand-in-hand with maternal mortality, sharing many of the same underlying issues: high poverty, low insured rates, lack of access to health care, and high gun violence. Mississippi, where more than half of single women with children live in poverty, is one of only 10 states that refused Medicaid expansion funded 90% by the federal government, not the state. Not coincidentally, it’s one of our worst states for infant mortality as well.
I’m a woman. If I could live or play anywhere, where should I consider?
All other factors about being equal, if I were a woman thinking about a career move, I’d pay attention to WalletHub’s analysis. But here are some of those “all other factors” that aren’t at all equal—because when a state doesn’t particularly care about women’s wellbeing, it shows up in multiple data sets.
We’ve had maternal and infant data the longest and the data couldn’t be clearer about where young moms are at greatest risk of death during pregnancy or birth. No thank you to Louisiana, Georgia, Indiana, New Jersey, and Arkansas and a few others. And several of those states are the same ones where the baby would also have a worse chance of living or suffering lifelong consequences of prematurity. If you live in Mississippi, you’d do better to have your baby in Turkey, which ranks 63rd out of 167 countries globally in overall healthcare but has a better infant mortality rate than Mississippi.
Yes, racism plays a role: if a demographic doesn’t really exist in the mid of those directing health education and training, than neither will that population’s health problems—whether that’s a racial or gender bias. One of the most stunning statements about that came from US Senator Bill Cassidy of Louisiana, a state where a third of the population is Black. Of Louisiana’s nation’s worst rate among moms, Cassidy said, “If you correct our population for race, we’re not as much of an outlier as it’d otherwise appear”. Never mind “not much of an outlier” doesn’t say much for how he thinks about Louisiana’s White women, either.
For women, it’s important to remember that gender and racial bias are connected; find one, you’re likely to find both. Whether Black or White, failure to focus on the issue keeps the US having third world maternal mortality rates. Despite spending more on health care than any other peer nation, the US is ranked 55th in the world in maternal mortality. Even Russia has a better ranking.
On the other end of the spectrum, women are most likely to die from heart disease in Mississippi. Women already die twice as often as men from heart attacks, in large part because women’s heart attack symptoms are different than men’s, and so can be missed if providers only know about men’s symptoms. That’s something research identified 20 years ago. Before then, doctors and hospitals couldn’t be blamed for not knowing that; we are far behind in research on health issues affecting women. While it takes 10 years for best practices to make it to the local level after research, most doctors and emergency rooms have integrated that information by now. The research clearly shows others still don’t or won’t.
Gender bias in emergency care won’t just be about heart attacks, either. Even today, only 25% of health research studies include women; you can’t identify sex differences if the research is only on one sex. As an example, new research shows men may be as much as three times more likely to receive appropriate immediate trauma care than women, e.g., from EMTs at the site of a car crash. Some states will integrate that in training; others won’t. I wouldn’t count on a state that already allows gender or racial bias to be among the first to train EMTs differently.
New studies also show young women now have a higher rates of lung cancer than men, and whether a state focuses on preventing those deaths plays out in those data. West Virginia, Arkansas, Oklahoma, and Tennessee are in the bottom ten states for women overall; they also have the highest rates of lung cancer among women.
If gender or racial bias already permeates a state’s health care training and practices, that will also be found in the most basic core of primary care. Among women, diabetes —which is linked with a whole host of other lifelong health problems—is highest in Alabama and Mississippi, again two of the worst states for women overall.
There are more, and more will show up.
Even today, only 25% of medical research includes women or identifies findings by sex—why it took so long to identify that women have different heart attack symptoms than men. There are likely many more sex differences in risk and treatment for illness that we don’t know than those we do. But one thing we do know from decades of research: some states consistently view women’s lives and health as more important than others. I’d be willing to be that when we do learn more, the 10 worst states for women’s health and lives now won’t suddenly show up in the top 10. And that’s why I don’t spend my vacations in the worst. Life is literally too short.